INTs: Needs - Function - Form
The Fuller Stocktake has triggered work on INTs. They are seen as central to more integrated working, at the level of neighbourhood and focussed on complex patients.
Integration is not a new idea in health or social care. In both sectors there is a long history of ‘integration’ initiatives, yet working in an integrated way remains a big challenge. Patient care is still often horribly fragmented and costly. The classic starting point in the NHS is to start with structure (FORM). Yet by jumping to structure first, we risk propagating the same old assumptions that that lead to ineffective models. To avoid this we need to follow: NEEDS > FUNCTION > FORM.
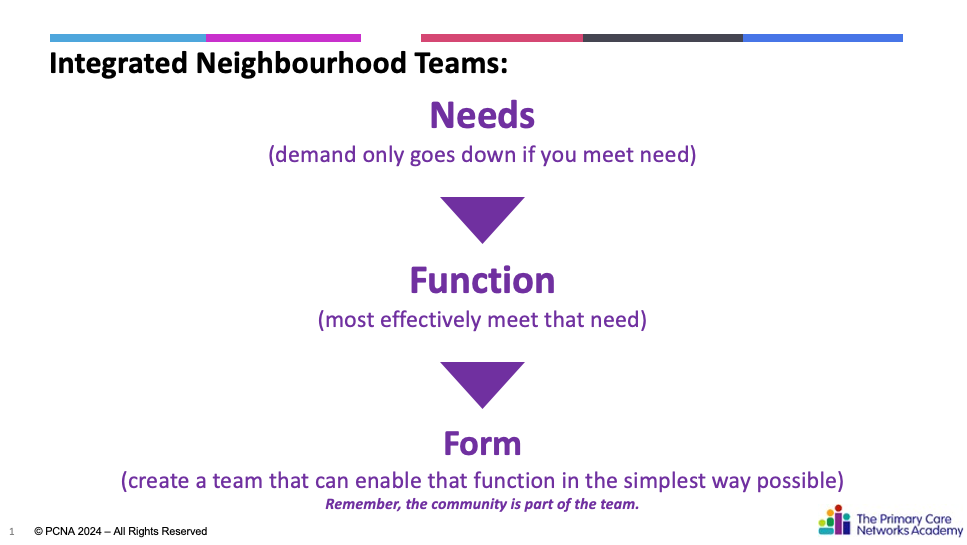
NEEDS: This means going beyond sticking plaster solutions. What is the need to be met in the eyes of the citizen? Who for? Is this just about Frailty and protecting A&E? What about young people with complex needs? Note our view of need is often corrupted by our systems of labelling and coding… Develop measures that actually matter and guide prototyping. Check this is actually INT work (new models have a habit of ‘sucking’ work up).
FUNCTION: How do we best meet that need? What kind of response would be required? What can we learn from cases? How effective have we been in the past? What patterns do we spot? In our systems of care that are dominated by rigid pathways, referring, deferring and professional gatekeeping, we have a lot to let go of……..
FORM: What form is required to achieve that function in the simplest possible way? Aim for more than coordinating professionals and services as this is often just a sticking plaster for fragmentation. What do we actually mean by MDT working? Is this just the convening of professionals to do their ‘bit’? Or are we working towards collective accountability, self-directed working and challenging boundaries?
In summary, we have a real opportunity to do something different with INTs – but only if we challenge assumptions on how they are approached and set up. Otherwise INTS will join the list of integration initiatives that fail to deliver on the promise. Worse still, fragmentation will continue to contribute to the huge Failure Demand (created by ineffective responses to need) that our care systems desperately need to avoid right now – the cause of up to 19%* of total GP demand.
What we do to help you
We can WORK WITH YOU directly on any of the things above, either hand-on to provide energy and support you and your organisation towards rapid change or just in a LIGHT TOUCH advisory role > contact@pcnacademy.org.uk
We also run INT Development programmes - see the dedicated page here
*Sources:
- General Practice Failure Demand Assessment - Develop Consulting
- Anderson-Wallace M & Downham N (2023); Improving Quality in Healthcare - Questioning the Work for Effective Change, Sage
© PCNA / Cressbrook Ltd 2024 – All Rights Reserved